

In veterinary medicine, the diagnosis must be an act that includes different stages, so it is as reliable as possible. Saying this seems frivolous, but we live in the era of the "laboratory diagnosis". What does this mean? It simply means that we frequently take as the fundamental (and sometimes the only) element the result of a supplementary laboratory test to make a diagnosis. This is, without a doubt, a mistake that leads us to confusion in a high percentage of situations.
Let us do something for the sake of order. Common sense tells us that we must be systematic when it comes to making a diagnosis, either of PCV2-related diseases or any other disease. Of course, we must follow a series of steps (Figure 1), avoiding as much as possible skipping any of them. We must start with an appropriate clinical diagnosis, with a thorough examination of the animals, looking for symptoms that help us in the diagnosis. In the case of systemic circovirosis, the symptoms are very well known (rapid body condition loss, coarse coat, diarrhoea, dyspnea, jaundice, etc.), but we must not forget that PCV2 can play a role in the respiratory complex inducing symptoms that are much more difficult to differentiate, or in other disorders, like reproductive failure, with stillborn or mummified foetus or piglets that are born weak, all of which are very unspecific symptoms as well. Of course, at this stage we must always include a good anamnesis and and take into consideration the historic records of that pig population (if we have them).
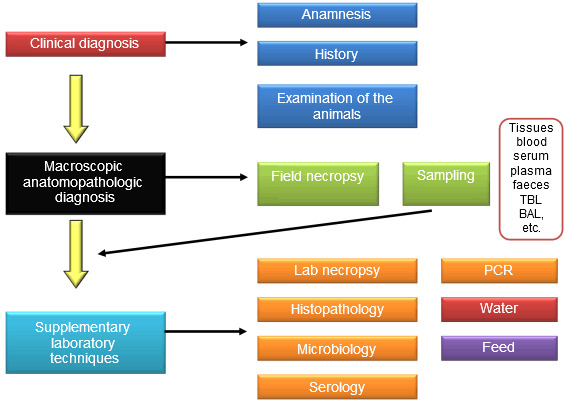
Figure 1. General diagram of the diagnosis process
The second step will be the anatomopathologic macroscopic diagnosis, based on the field necropsy findings.
Unfortunately, any disease process in a group of pigs normally implies a certain mortality rate. A dead pig is a potential loss of benefit that we can minimize by obtaining its only asset: information about the disease that killed the animal. In the case of PCV2 (when the clinical profile is that of PMWS) we can see enlarged lymph nodes (especially the superficial inguinal and mesenteric lymph nodes), interstitial lung oedema that suggests an interstitial pneumonia, concomitance of lesions typical of PDNS, etc., without forgetting that the virus can also cause reproductive disorders in which we may find stillborn or weak-born piglets, or mummified foetuses on which we can conduct a necropsy in order to see visible heart disorders. Necropsy is the only way of giving some value to a dead pig.
These first two steps will give us a presumptive diagnosis, which is sometimes enough for implementing a treatment, but in other cases it will need a confirmation. Unfortunately, PCV2-related diseases are not among those inducing clinical signs or macroscopic lesions that are absolutely distinguishable from other diseases. The time to turn to the supplementary laboratory tests has come.
We will use samples taken during the clinical inspection or necropsy (bear in mind the time elapsed from the death of the animal, because sometimes it is worthwhile to euthanize an animal). Among all the laboratory techniques, the most used ones for diagnosis are, without a doubt, histopathology (including specific techniques that are based on staining as, for instance, immunocytochemistry), serology (especially those techniques that distinguish between IgG and IgM and allow us to deduce if the disease is at an initial or late stage (see figure 2), and molecular techniques, including PCRs (the classical and the real-time PCR, that allows to quantify the amount of PCV2 ADN copies present in the sample) and in situ hybridization.
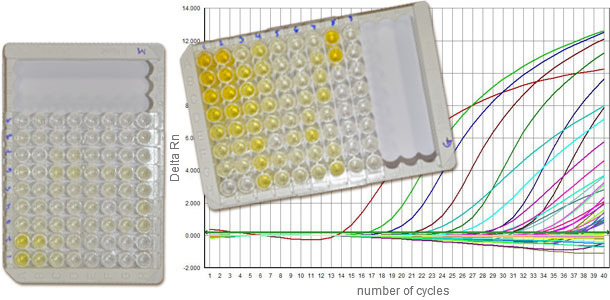
Figure 2. Serology tests against PCV2 enable to characterize the IgM and IgG response, helping us to deduce at which moment of the infection process are the animals. The q-PCR gives information about the viral load.
All of them have advantages and weak points. Of course, histopathology is going to help us to determine the presence of microscopic PCV2 characteristic lesions in the lymphoid tissue (lymphocytic depletion and granulomatous inflammation), lung (interstitial inflammation), intestine (granulomatous enteritis) or even in the heart of the foetuses (fibrotic and/or necrotizing myocarditis). The immunocytochemistry and the in situ hybridization help us to ascertain the association between the virus andd the lesions in the different tissues. The PCRs help us to ascertain the presence of the virus, and they are very useful for ascertaining the presence of viraemia or the viral load (in the case of the foetuses, it is accepted that more than 107 copies of PCV2 genome/500 ng of extracted DNA clearly show an infection with PCV2), but they do not allow us to ascertain that the virus is related to the characteristic lesions (one of the three Sorden’s criteria –together with the clinical symptoms and the compatible histological lesions- in order to diagnose a case of PMWS). Furthermore, a positive serology reflects a contact with the virus (closer or more distant in time with respect to the moment of the sampling), but it does not give us much more information. Another use is the evaluation of the vaccinations, although this can also be somehow confusing if we only base ourselves on the serologies, because the fact of having a negative serology after a vaccination does not imply that the animal is not protected against the virus. And it can even be used for ascertaining the presence of PCV2 specific IgG in the peritoneal fluid of the stillbirth foetuses, although it is not clear that this sign is associated with an intrauterine infection with PCV2.
Once we have the laboratory results we will combine them to the presumptive diagnosis and we will be able to obtain a confirmed diagnosis (if it is possible with the results obtained with the aforementioned tests, because sometimes they are not concluding).
We must always bear in mind that skipping steps in this diagram always entails the risk of making mistakes. Trying to diagnose a process by means of PCR or serology without even having carried out a good examination of the animals (sometimes even without using a thermometer) or some necropsies is a mistake that we must avoid at all costs, for efficacy and financial reasons. A laboratory test costs money. A field necropsy makes us recover a part of the financial loss caused by the death of the animal. We must not forget that.

