

Assays available:
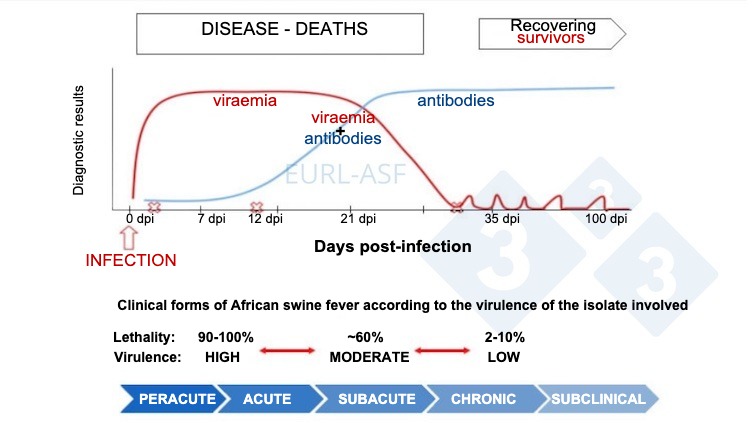
The following graph shows changes in concentration (Y-axis) over time (X-axis) of different analytes used in assays. After exposure, viremia will start within 1 or 2 days of exposure and last for about 3-4 weeks. Seroconversion (antibody detection) usually occurs 14 days post exposure and lasts for many months or years.
Polymerase chain reaction (PCR)
- Detects presence of specific sequence of viral nucleic acid (DNA)
- Sample types: serum, whole blood or tissues
- Pros:
- Most sensitive and preferred method for detecting agent
- Moderate cost
- Can often do pooling of samples to lower cost while minimizing loss of sensitivity
- Cons:
- Requires proper primers
Hemadsorption test (HAT)
- Detects presence of virus through attachment of erythrocytes to the external (cytoplasmic) membrane of ASFV‐infected porcine macrophages
- Sample type: Serum or plasma
- Pros:
- One of the standard reference tests
- Cons:
- A few field strains do not induce hemadsorption and negative results usually require confirmation via PCR
Antigen detection enzyme-linked immunosorbent assay (Ag-ELISA)
- Detects presence of agent
- Sample types: usually whole blood and possibly other specific tissues (must follow kit recommendations)
- Pros:
- Commercial kits available
- Relatively inexpensive
- Cons:
- Much lower sensitivity than PCR
- Pooling of samples not recommended
- Negative results usually require confirmation via PCR
Antibody detection enzyme-linked immunosorbent assay (Ab-ELISA)
- Detects presence of antibodies
- Sample types: serum or plasma
- Pros:
- Animals remain positive for several months to years
- Can be used in chronic cases
- Can be used in low-virulence/sub-clinical cases
- Seroconversion can occur in 7-10 days
- Currently no commercial vaccines are available to confound interpretation of positive results
- Cons:
- Takes 7 to 10 days for animals to become seropositive
- Unable to differentiate maternal antibodies vs exposure
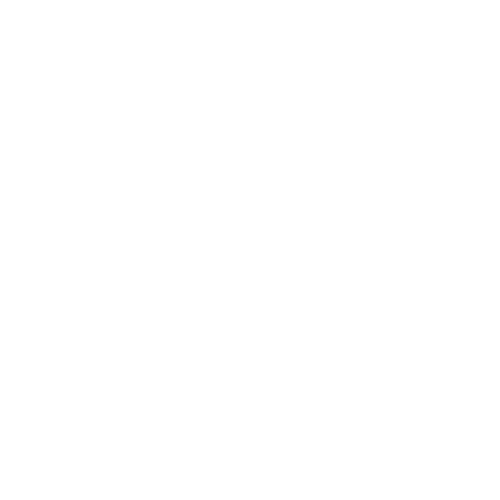
Indirect fluorescent antibody (IFA)
- Detects presence of antibodies
- Sample types: serum or plasma
- Pros:
- Confirmatory test for unexpected ELISA positive samples
- Cons:
- Requires animals to be have been infected for at least 1 week
- Not feasible for large number of samples
- Results impacted by virus isolate used for assay
- Reliability is highly dependent on technician skills
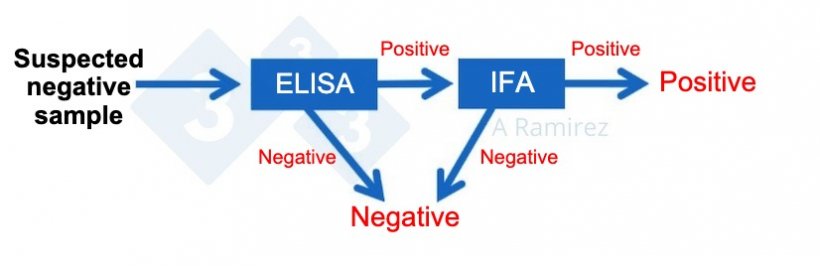
Indirect Immunoperoxidase test (IPT)
- Detects presence of antibodies
- Sample types: serum or plasma
- Pros:
- Confirmatory test for unexpected ELISA positive samples
- Cons:
- Requires animals to be have been infected for at least 1 week
- Not feasible for large number of samples
- Results impacted by virus isolate used for assay
- Reliability is highly dependent on technician skills
Result interpretation:
Often multiple assays are needed to provide a better interpretation of ASF diagnostics.
Table 1. Interpretation of the ASF diagnostic results. Source: European Union Reference Laboratory for African swine fever.
| Assay | Result | Most likely scenarios |
|---|---|---|
| PCR | Weak (Ct>35) | The animal was recently infected and it has not yet seroconverted (<7 days). Clinical signs may not be evident. |
| Ab-ELISA | Negative | |
| IPT | Negative | |
| PCR | Positive | The animal was recently infected, develop clinical signs and is initiating the seroconversion (7-10 days). |
| Ab-ELISA | Negative | |
| IPT | Positive | |
| PCR | Positive |
a) Infection in course. The animal is still viraemic with clinical signs and has already seroconverted (>10 days). b) Reinfection of an animal with preformed antibodies from a previous infection (recovered, surviving pig). IPT titer will offer information on the time of infection. |
| Ab-ELISA | Positive | |
| IPT | Positive | |
| PCR | Weak (Ct>35) or Negative |
a) Past infection. The animal has recovered from acute or subacute infection and may not present clinical signs. b) The animal was infected with an attenuated strain (with or without clinical signs). c) Reinfection of an animal with preformed antibodies from a previous infection (recovered, surviving pig). IPT titer will offer information on the time of infection. |
| Ab-ELISA | Positive | |
| IPT | Positive |
PCR
- Positive: Virus is present; current infection
- Negative: Negative or virus could have been missed if testing occurs late after infection
HAT
- Positive: Virus is present; current infection
- Negative: Negative, infection with a non-hemadsorption isolate, or virus could have been missed if testing occurs late after infection. Must confirm negative with PCR
Ag-ELISA
- Positive: Virus is present; current infection
- Negative: Negative, virus present but at low concentrations, or virus could have been missed if testing occurs late after infection. Must confirm negative with PCR
Ab-ELISA
- Positive: Maternal antibodies or past exposure (>7-10 days) to wild-type virus
- Negative: Negative or wild-type infection too early to detect
IFA
- Positive: Maternal antibodies or past exposure (>7-10 days) to wild-type virus
- Negative: Negative or wild-type infection too early to detect
IPT
- Positive: Maternal antibodies or past exposure (>7-10 days) to wild-type virus
- Negative: Negative or wild-type infection too early to detect
Scenarios
Important to note that some countries may require approval by federal authorities before any testing for ASF can be done.
Suspected acute ASF outbreak in any age pigs
- Collect whole blood from multiple affected animals and test via PCR; sample pooling may be considered
- Collect spleens and tonsils from dead pigs and test via PCR; sample pooling may be considered

Suspicion of chronic ASF circulation in any age pigs with no mortalities
- Collect whole blood from 30 pigs with clinical signs (targeted sampling) or randomly sampled (no clinical signs) and test via PCR (sample pooling may be considered) and test individually with Ab-ELISA






